
Starting from roughly around the early part of the COVID-19 pandemic, there has been a surge in exposure and interest in strength and strength training, especially for older adults. This is excellent because it’s something we strength training folks have known and have been trying to tell anyone that cared to listen to for the longest time: that everyone should strength train to get stronger because strength is important to life and underlies many physical attributes like health (both physical and mental), quality of life, physical independence, and sports performance.
Strength is the foundation. Everything else builds on it.
At Hygieia, we talk a lot about the importance of getting stronger. Not for appearances, but for health, physical independence, and quality of life as you get older. Muscle doesn’t just pull on your bones to enable you to move around. It is metabolically active tissue that supports your joints, regulates your metabolism, and keeps you physically capable of doing the things you want to do. Losing muscle mass, which happens to everyone who doesn’t actively work against it, is one of the most significant and underappreciated threats to long-term health.
So if you want to find out where you stand in terms of your strength levels, which is a strong predictor of your future physical outcome, how can you measure it? Using exercises to test for strength like a 1RM squat or deadlift isn’t practical for the general population because there’s a high skill component to it and difficult to administer. Getting someone who has zero experience with the lifts and is physically deconditioned to do that is not only unwise, but it can also potentially be dangerous as well. We need something that’s simple, doesn’t require a specific skill or practice, is quick to administer, is reproducible, and can be used over a very broad population. Something like the standing vertical jump test to test for neuromuscular efficiency and explosiveness. There’s a test for that and it’s the grip strength test.
Grip strength as a proxy for overall strength
When we measure grip strength, we’re not exactly how hard you can squeeze per se. It’s a proxy – a simple, quick to administer, and inexpensive test that can be broadly used to measure your strength. How hard you can grip reflects your overall musculoskeletal health. Your grip reflects the general state of your muscles, your neuromuscular function, your physiological reserve and is a reliable predictor of future health outcomes.
If those systems are in good shape, your grip tends to be strong. If they’re declining, your grip reflects that too.
What the research says
The evidence linking grip strength to health outcomes is substantial.
All-cause mortality
Studies have consistently found that weaker grip strength is associated with higher all-cause mortality. A 17-year follow-up study of thousands of adults found that every meaningful decline in grip strength corresponded to a measurably higher risk of earlier death from almost any cause, regardless of age, sex, or lifestyle factor [1]. The effect was consistent across age groups and both sexes.
Cardiovascular health
The cardiovascular findings are particularly interesting. Studies have found that grip strength was actually a stronger predictor of dying from heart disease than systolic blood pressure [2].
Dementia and cognitive decline
Most people only consider the physical benefits when training, but actually, there are a lot of mental benefits to it as well. We think of cognitive health as a brain issue, but the research increasingly points to the whole body being involved. The link to cognitive decline is also well-established. The UK Biobank study of nearly 190,000 adults found that lower grip strength was associated with greater risk of developing dementia over a follow-up period of about 12 years [3].
None of this should be surprising when you dive deeper into what muscle does. It does way more than just pulling on your bones to enable you to move around. It’s an active organ that communicates with your cardiovascular system, your brain, and your immune system. When your muscle mass and strength decline, the downstream effects are systemic.
Before I carry on with this article, I just want to mention the inspiration behind it. This article started, as many things do at Hygieia, because of our conversations with our clients or what we observe when coaching.
One of our clients was resting between sets and scrolling on her phone on an online shopping site. She came across a digital hand dynamometer and thought it looked interesting. She bought one for herself and, very generously, got one for us too. When she brought it in, we started testing ourselves and our clients out of curiosity. Then it occurred to me that since we know that a strong grip strength has a proportional correlation to positive health outcomes, and most, if not all, of our clients are here to improve their health, well-being, and quality of life by getting stronger, I thought it’d be interesting to see how our clients stack up, where they are as compared to the age-adjusted average grip strength. So here we are.

So, thank you Swat for the hand grip dynamometer, which inspired this article.
How our clients stack up
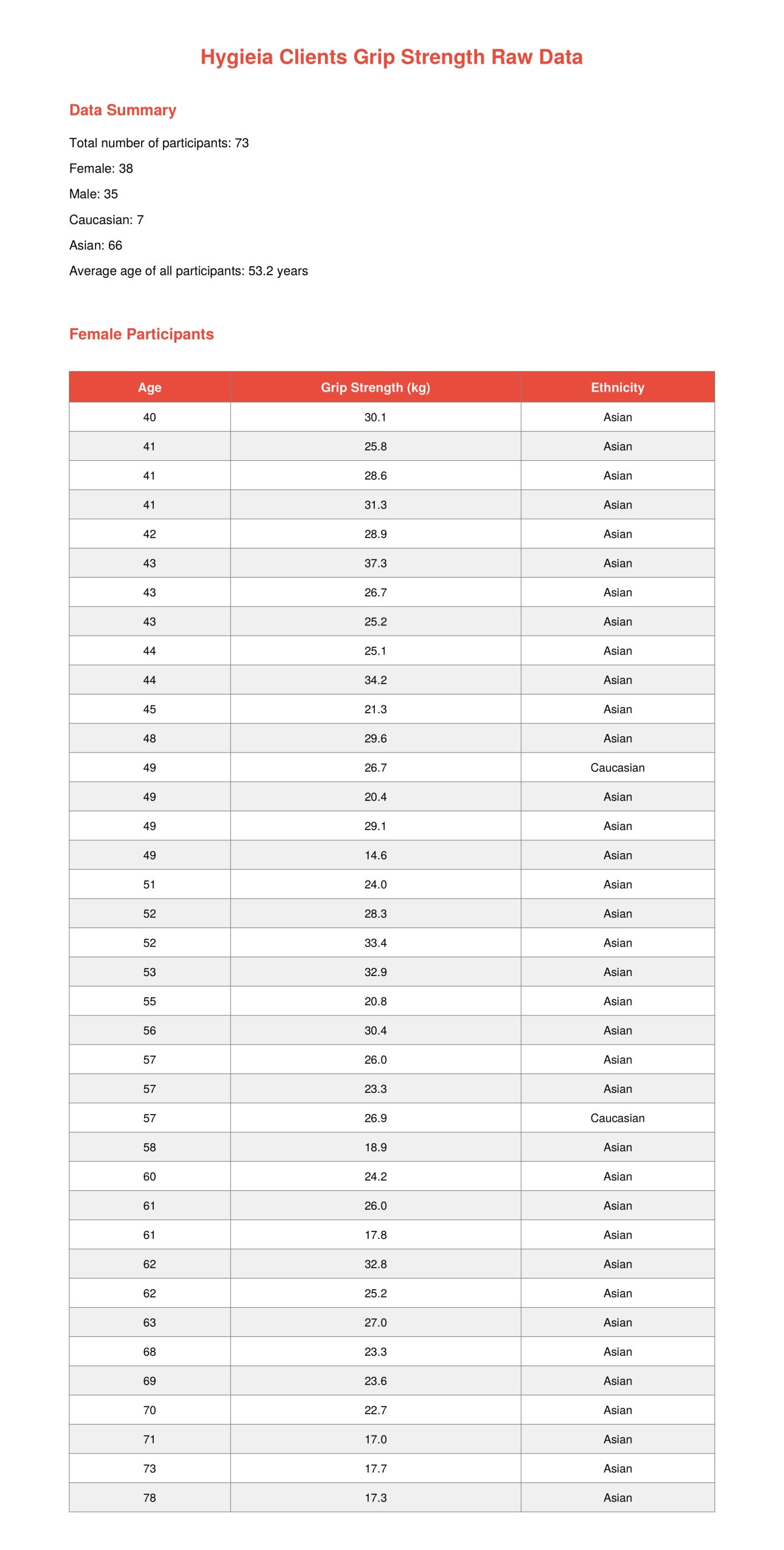
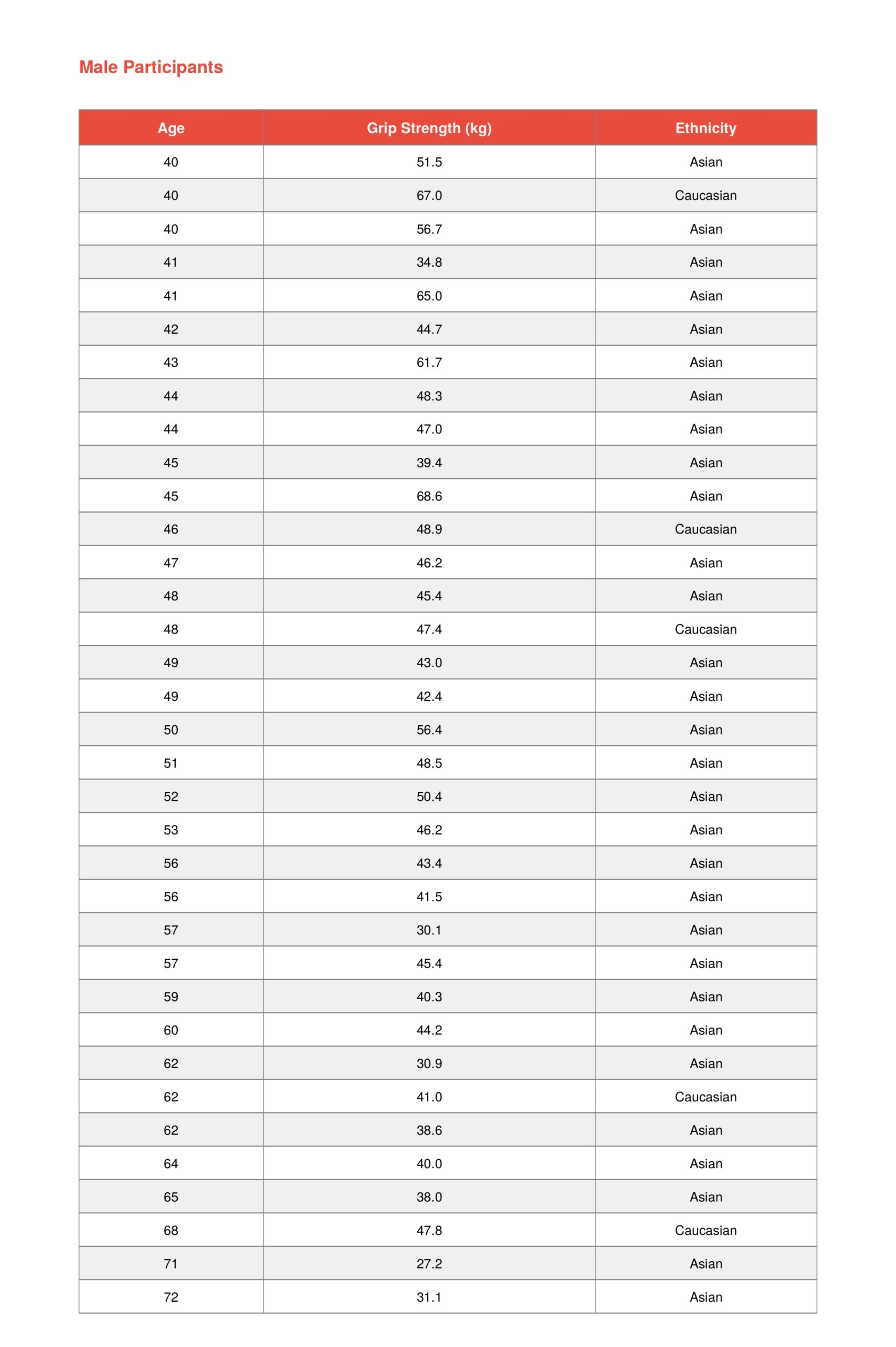
Coincidentally, a day after Swat gave us the dynamometer, Marvin mentioned that the dynamometer he bought had been delivered. I took that as a clear sign that the universe was coming together to tell me that this article was meant to be. Over the next two weeks, we measured every client over 40 years old that came in to train at both our outlets. It was a mix of clients that have trained with us for weeks or months to years. In total, we measured the grip strength of 73 clients and out of the 73, 7 were Caucasian. The remaining 66 clients were of Asian descent. We then compared the results against published normative data for Asian adults, drawn from two large population studies covering tens of thousands of people [4, 5].
The results were clear. Across every age group, our clients came out above the general population average. Men in their 40s averaged about 10kg above the norm. Women in their 60s averaged 4.5kg above. Even in the older age groups where population averages drop sharply, our clients had above average grip strength.
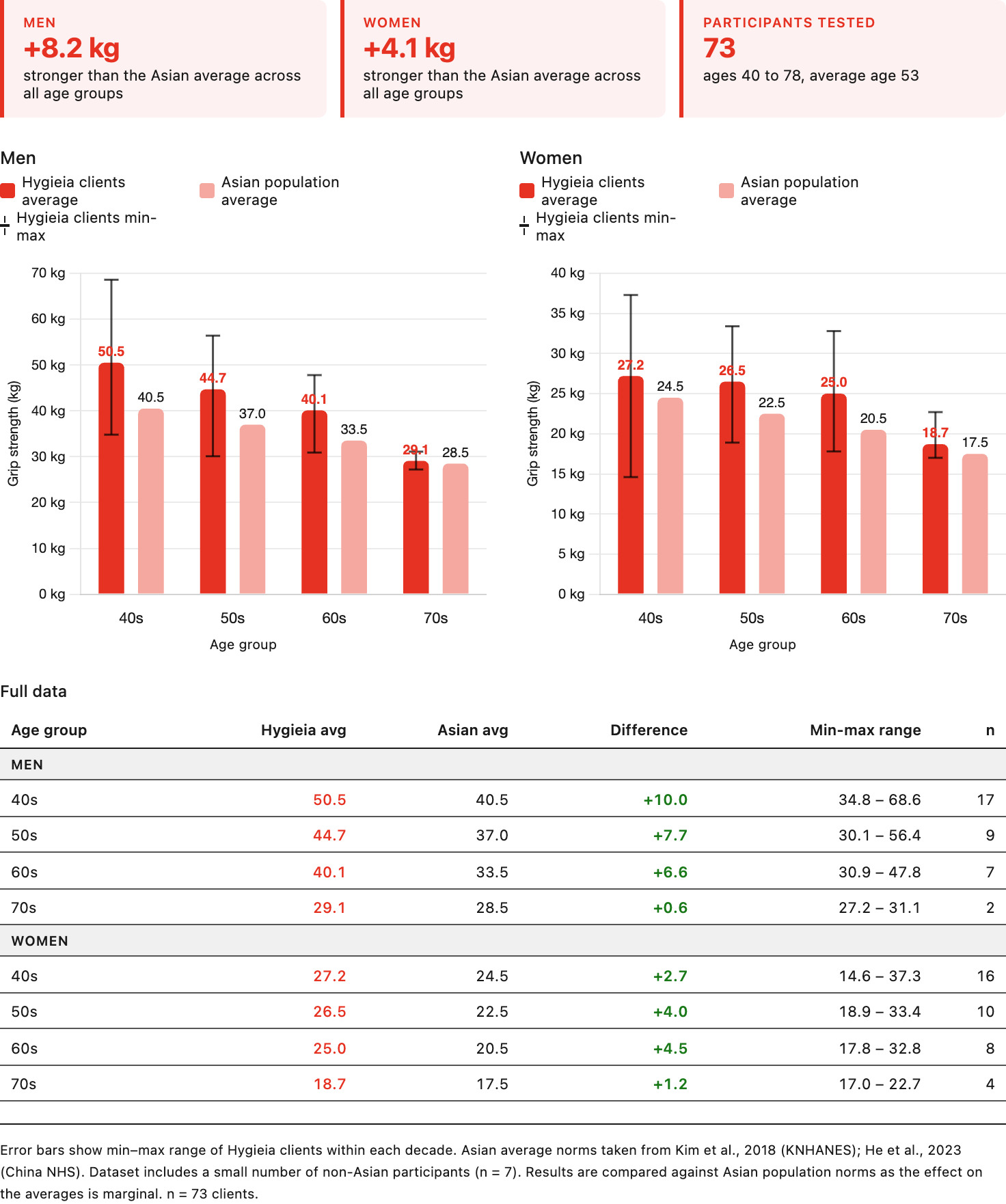
To be honest, this isn’t surprising to us. We expected our clients who have been consistently getting stronger over months and years to be stronger than their average counterpart and, as a result, have a higher than average grip strength.
Don’t train your grip for this test
When we shared the results with our clients, a few of them joked that they were going to start doing grip-specific training to improve their numbers in the hope of getting better health outcomes. While I know where the thinking behind the comment is coming from, doing so would completely defeat the purpose of the test.
Grip strength is a useful test because it reflects your general physical condition rather than a specific trained skill. It’s but a proxy. If you start training grip specifically to score well on a dynamometer test, you’ll improve the number without improving the underlying thing the number is supposed to represent – your cardiovascular health, your overall muscle mass and strength. None of that changes because you’ve been specifically training your grip.
The value of these proxy measurements depends entirely on them being incidental rather than trained. The moment you specifically prepare for the test, you’ve corrupted the signal.
What we do at Hygieia is simple: just the basic barbell lifts like the squat, press, deadlift, and bench press, and accessory exercises like chin-ups. We select these exercises because they train the entire body as a system and when the numbers of these lifts go up, you systemically get stronger as a whole. And that’s why our clients produce the numbers on the grip strength test that they did.
Where do you stand?
The Asian Working Group for Sarcopenia (the body that sets clinical standards for age-related muscle loss across Asia) defines low grip strength as below 28 kg for men and below 18 kg for women [6]. Falling below these thresholds is associated with significantly higher risk of falls, loss of physical independence, hospitalisation, and early mortality.
These aren’t arbitrary numbers. They represent the point at which the research consistently shows health risk rising to a clinically significant level.
The grip strength test takes a few seconds to perform. If you haven’t done it, it’s worth doing to see where you stack up. Compare your result to the averages for your age and sex. If you’re above average, that’s a good sign. If you’re below average, or below the low grip strength thresholds above, perhaps it’s time you start seriously considering starting strength training.
References:
1. Svinøy, O. E., et al. (2016). The association of grip strength from midlife onwards with all-cause and cause-specific mortality over 17 years of follow-up in the Tromsø Study. Age and Ageing. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC5136688/
2. Bohannon, R. W. (2019). Grip strength: An indispensable biomarker for older adults. Clinical Interventions in Aging, 14, 1681–1691. https://pmc.ncbi.nlm.nih.gov/articles/PMC6778477/
3. Duchowny, K. A., et al. (2022). Associations between handgrip strength and dementia risk, cognition, and neuroimaging outcomes in the UK Biobank cohort study. JAMA Network Open, 5(6), e2218314. https://jamanetwork.com/journals/jamanetworkopen/fullarticle/2793510
4. Kim, M., & Shin, C. (2018). Muscular grip strength normative values for a Korean population from the Korea National Health and Nutrition Examination Survey, 2014–2015. PLOS One, 13(8), e0201275. https://journals.plos.org/plosone/article?id=10.1371/journal.pone.0201275
5. He, H., et al. (2023). Normative values of hand grip strength in a large unselected Chinese population: Evidence from the China National Health Survey. Journal of Cachexia, Sarcopenia and Muscle, 14(3), 1312–1321. https://pmc.ncbi.nlm.nih.gov/articles/PMC10235885/
6. Chen, L. K., et al. (2019). Asian Working Group for Sarcopenia: 2019 consensus update on sarcopenia diagnosis and treatment. Journal of the American Medical Directors Association, 21(3), 300–307. https://www.jamda.com/article/S1525-8610(19)30872-2/abstract